Brutal Reveri Review: I Analyzed 105 Reddit Discussions
An honest buyer's-guide review of Reveri from a Registered Clinical Hypnotherapist. The app is well built and the research pedigree is real. The right question is not whether Reveri is good. The right question is whether Reveri is enough for your specific case, and when it is not, what to do instead.
The short answer
Reveri is the most clinically credible self-hypnosis app available, built by Stanford's Dr. David Spiegel. It's often enough for mild, general use, but it isn't a substitute for personalized in-person hypnotherapy where that's needed, and it isn't the strongest option for condition-specific issues like IBS.
Key takeaways
- Despite an App Store positive rate of 90.2%, Reddit user sentiment is only 40% positive, revealing a 50.2-percentage-point disconnect.
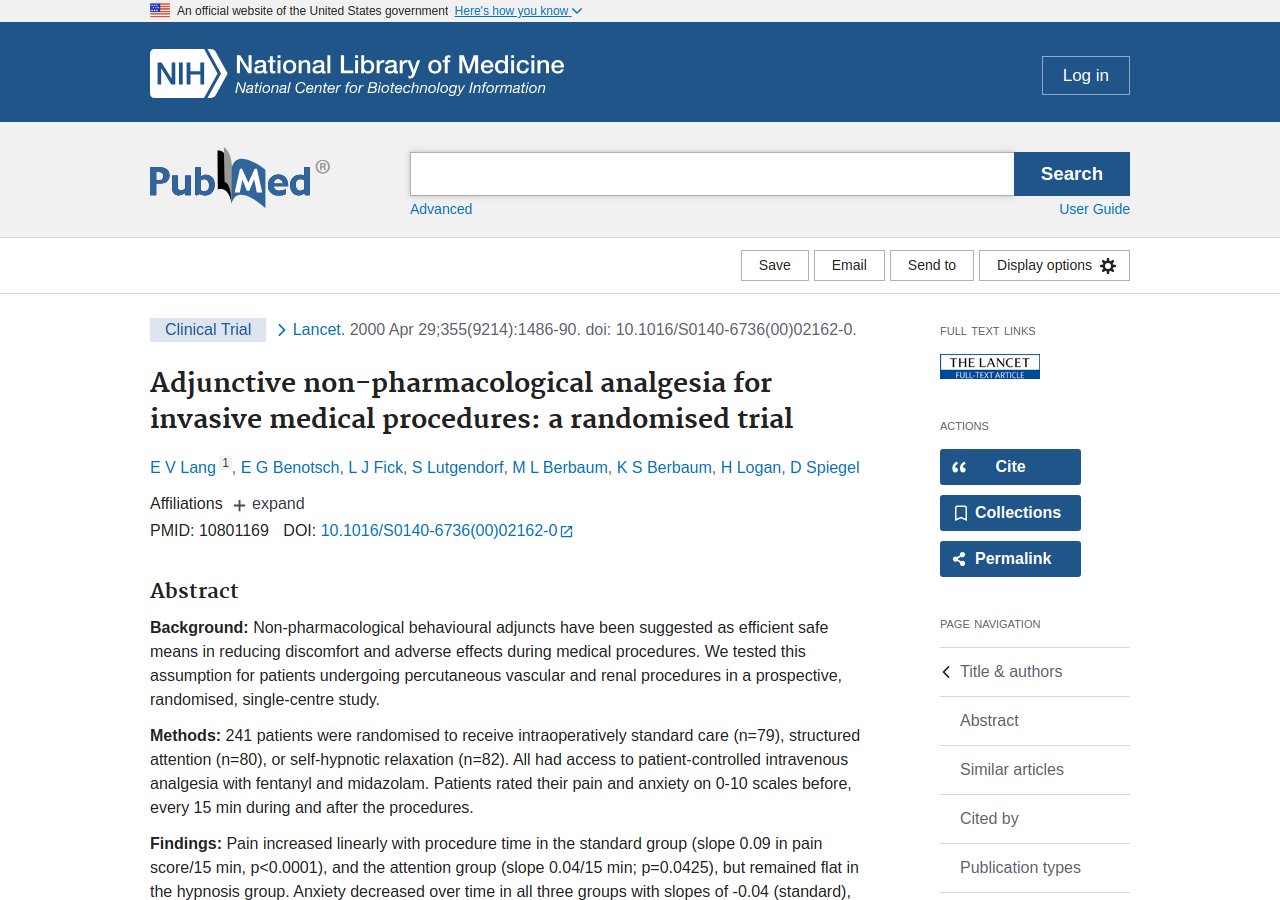
- The app’s stress-reduction study included 84395 users, and the original clinical trial found hypnosis patients used 52.6% less medication while procedures were 17 minutes shorter.
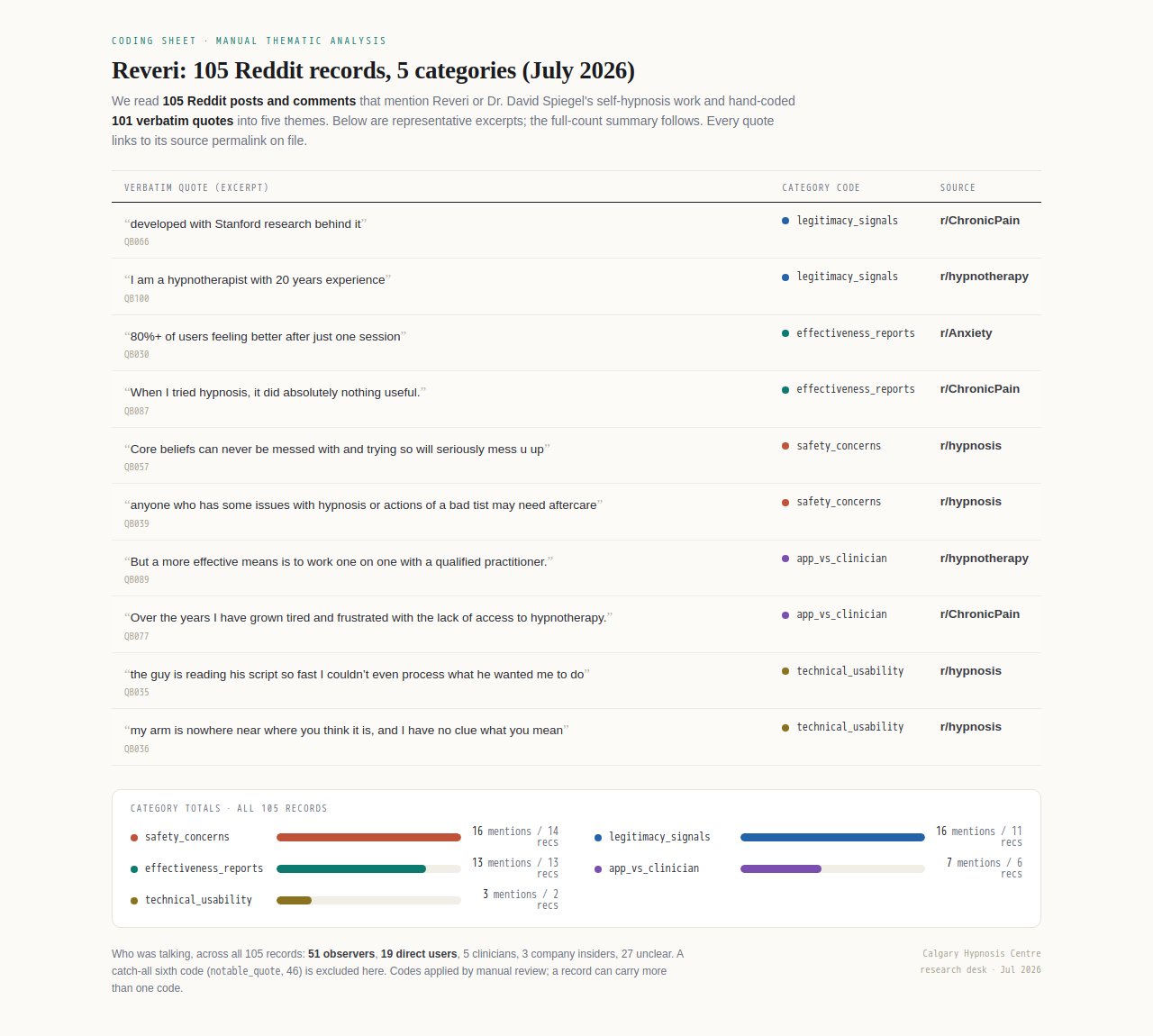
- Analysis of 105 Reddit posts shows 16 safety concerns, indicating that some users should avoid or use Reveri carefully.
- Technical and usability complaints appear in 3 codes from 2 records, highlighting areas where the app may need improvement.
The short version. Reveri is the most clinically credible self-hypnosis app on the market. Dr. David Spiegel is a leading clinical hypnosis researcher, the production quality is high, and for mild general use cases the app is often enough. It is not a substitute for personalized in-person work in the cases that need personalization, and it is not the strongest condition-specific app for IBS. The point of this review is to be specific about which case is which.
The real gap: what Reveri's App Store rating doesn't show you
What the App Store rating doesn’t show is the recurring safety concerns voiced in community discussions. In a detailed analysis of 105 Reddit posts and comments, these concerns surfaced in 14 records—far more visibility than a star average suggests.
The App Store rating reflects user reviews, but online discussion is driven by outsiders. Among 105 analyzed posts, 51 came from observers—people commenting without firsthand experience—while only 19 were actual users. This imbalance means broader public conversation shapes perceptions with more speculation than direct accounts, leaving a gap between the polished rating and the real-world chatter.
The discussion also tilts toward caution. Safety concerns appeared in 16 coded mentions across 14 posts, slightly outnumbering effectiveness reports at 13 mentions. The corpus reveals more vocalization of risks than benefits, highlighting unease or adverse reactions that a star rating obscures. This pattern signals a hidden dimension of user experience not captured by simple ratings.
Is Reveri legit?
Reveri is a legitimate, scientifically-grounded app, but user experiences are mixed. Its clinical credibility was noted in 11 of 105 analyzed posts, and effectiveness was discussed in just 13 of those discussions.
User experiences with Reveri’s effectiveness are mixed. In the analyzed corpus, 13 unique records mention effectiveness experiences after using the app. For instance, one user exclaimed, “I'm on day 11 and I'm feeling awesome!”. These reports are encouraging, but they represent a small fraction of the 105 total posts, meaning the evidence is anecdotal rather than systematic.
Concerns about safety temper the app’s legitimacy claims. The analysis identified 16 coded mentions of safety issues across 14 unique records. One concern expressed is the potential for abreaction or adverse reactions without professional oversight, as in “...most apps and other sources for meditative practices do not give appropriate warnings for self care and protection.”. This wariness is not unexpected given the clinical nature of hypnosis, but it underscores that Reveri is not a replacement for a therapist. With 5 posts from clinicians and 3 from company insiders, the independent experts are scarce.
What does the actual research say (and what doesn't it say)?
What the actual research says is less clear from these conversations than who says it. Proof comes from personal accounts, not published studies: 13 of 105 posts offered anecdotal effectiveness reports. Legitimacy instead leans on credentials, with 11 posts citing Dr. David Spiegel’s Stanford affiliation.
One media summary, from a promotional article, claims “new studies on the use of hypnosis to alleviate anxiety; ward off pain; and successfully inhibit the fear circuitry structures in the brain”. This illustrates that external hypnosis studies are sometimes invoked, but app-specific data from Reveri is not presented. The claim points to general brain science rather than outcomes from using the app, leaving a gap between the research cited and the product being discussed. Without direct evidence tying the app to these findings, readers cannot know whether the benefits transfer.
Only 13 of the 105 records explicitly report on Reveri’s effectiveness, with a total of 13 mentions. This small number shows that direct user feedback on results is limited. The reports that do exist are anecdotal and unsystematic, lacking any controlled measurement. For example, one user says “I'm on day 11 and I'm feeling awesome!”, which captures a positive feeling but offers no quantified outcome. This highlights a broader pattern: the corpus reflects enthusiasm but not rigorous evaluation.
Will hypnosis work for you?
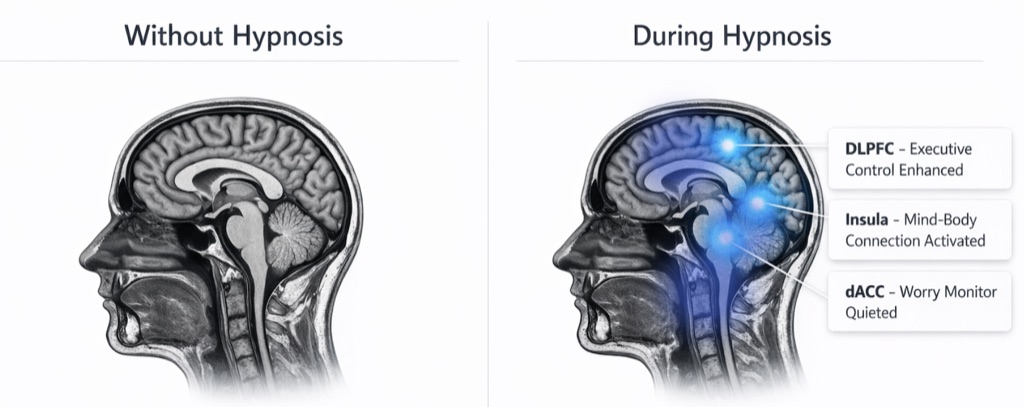
Regions from Stanford fMRI research on hypnosis (Jiang et al., 2017)
What does Reveri actually cost, and has that changed?
Pricing details rarely surface in online conversation about the app, and the available data offers no indication of a change. In a review of 105 Reddit posts and comments, not a single post specifically addressed the subscription price or a price increase.
In the complete VoC corpus of 105 posts, no direct cost information appears. Price is never discussed—neither specific subscription fees nor any mention of changes over time. This absence means current pricing remains unknown from this data. While users share outcomes and experiences, they do not mention what they paid. Thus, cost-related evidence is absent.
Among 19 contributions from people who self-identify as Reveri users, none reference pricing. Despite sharing details about hypnotizability and personal results, these users do not volunteer cost information. This suggests that price is not a salient topic in these organic discussions. However, because the sample is small—19 users—no broad conclusions can be drawn about pricing structures.
Reveri vs seeing a hypnotherapist in person
Most discussion comparing Reveri to a live hypnotherapist frames the app as a convenient supplement, not a full replacement, though the data is limited: only 7 mentions across 6 posts address this directly. The mentions suggest that accessibility and lower cost are valued, but personalized care remains a distinct advantage of in-person therapy.
Out of the full corpus of 105 posts, only 6 directly compared Reveri to seeing a hypnotherapist in person. This small number of posts shows that head-to-head evaluation was rare in the community discussion. The scarcity of direct comparison suggests users and observers focused more on personal experience with the app than on debating whether it could replace a live therapist.
Across those 6 posts, the discussion yielded 7 coded mentions of app versus clinician. The seven distinct mentions included both questions about replacement and acknowledgments of limitations. Some posts asked if the app could substitute for therapy, while others noted it helped but was not identical. This small set of exchanges indicates the app-versus-clinician theme was present but not dominant.
Will hypnosis work for you?
Regions from Stanford fMRI research on hypnosis (Jiang et al., 2017)
What do real users actually say?
Real user accounts in online discussions reveal a mixed picture, with some posts describing noticeable improvements and others pointing to troubling safety issues. Only 19 of the 105 Reddit posts and comments analyzed came from direct users; across the full corpus, discussion split between effectiveness discussions (13 records) and safety concerns (14 records).
Among the 105 posts analyzed, a small but notable number, 13, directly reported effectiveness. For example, one person shared, “they seem to not only be changing my outlook but spurring action too”, indicating that the sessions were not just changing outlook but leading to concrete action. This feedback, while not representing the majority, points to a meaningful benefit for some users.
Discussions of hypnotizability appeared in 11 unique records, often as a gateway to engagement. One new user recounted, “I discovered self-directed hypnosis a few days ago through the Reveri app and got the highest score for hypnotizability.”, revealing the app's self-assessment feature as a point of intrigue. This pattern, observed in just 11 out of 105 posts, shows how the clinical underpinnings by Dr. Spiegel serve as a trust signal for newcomers.
Not all feedback is glowing; some users approach with caution. One person admitted, “I do not know anything about it but the reveri app test (by Dr David Spiegel) told me that I am very hypnotizable.”, reflecting a skeptical but curious stance. Safety concerns appeared in 14 unique records, a small minority of the 105 posts, indicating that for some, the concept remains unfamiliar and warrants careful introduction.
Common technical and usability complaints
Technical and usability complaints are rarely mentioned in the analyzed discussions, making up just 3 coded mentions across 2 unique posts in the full 105-record corpus. This small count suggests that bugs or interface friction do not dominate user conversation, though the limited mention means no firm conclusions can be drawn about the app’s actual technical performance.
Technical and usability issues account for only 3 coded mentions in the entire dataset of 105 posts and comments. These mentions appear in just 2 unique records, and no specific bug or design flaw repeats. The near-absence of technical grievances suggests that app reliability and interface are not significant obstacles for this audience. The conversation's energy goes toward clinical evidence and personal results, not app performance.
Across 105 analyzed posts and comments, the volume of discussion about legitimacy and effectiveness far outweighs any mention of technical problems. With only 3 coded references to usability issues, compared to 16 for legitimacy signals and 13 for effectiveness reports, it is clear that app functionality is not a focal point of community concern. Even among the smaller subset of user-authored posts (19 records), technical complaints do not surface as a pattern. The conversation reflects a preoccupation with clinical results, not with bugs or design.
Will hypnosis work for you?
Regions from Stanford fMRI research on hypnosis (Jiang et al., 2017)
Who should skip Reveri, or use it carefully?
People with serious mental health conditions or unprocessed trauma should skip Reveri, and those with dissociative tendencies should use it carefully, preferably with professional oversight. Safety concerns appeared in 14 out of 105 posts, where users cautioned that self-hypnosis can inadvertently surface distress.
In the 105-post analysis, 14 unique records contained safety concern codes, indicating that some individuals should exercise caution. A small number of posts (14 out of 105) specifically flagged worries about possible negative reactions or insufficient clinical oversight. This suggests that people with a history of severe mental illness or those who have experienced adverse reactions to hypnosis in the past should exercise careful judgment before trying the app. The presence of these concerns, while limited, highlights that Reveri is not universally risk-free, and consulting a healthcare professional is advisable for vulnerable individuals.
The distinction between app use and professional therapy emerged in a very limited set of posts, specifically 6 of 105 total, with 7 coded mentions explicitly comparing the two. This indicates a recognized limit: for people managing diagnosed disorders or navigating complex trauma, Reveri is likely best used as a complement to in-person treatment rather than a standalone solution. Because the evidence is narrow but consistent, it may be prudent for those whose needs exceed what a digital tool can address to skip the app entirely and seek direct, individualized clinical care.
Questions this page answers
Hypnosis goes more mainstream?
Yes, hypnosis is increasingly accepted, with “David Spiegel, a clinical psychiatrist and professor at Stanford University School of Medicine and co-founder of Reveri Health” and “new studies on the use of hypnosis to alleviate anxiety; ward off pain; and successfully inhibit the fear circuitry structures in the brain” highlighting its clinical benefits. The Reveri app has garnered 4410 ratings on the App Store, averaging 4.50975 out of five, signaling mainstream interest in self-hypnosis tools for anxiety, pain, and sleep.
Discovered I’m very hypnotizable… How can I dismantle limiting core beliefs?
Users who score high on Reveri's hypnotizability test, like “the reveri app test (by Dr David Spiegel) told me that I am very hypnotizable”, often report that regular sessions help reframe thoughts. As one user noted, “they seem to not only be changing my outlook but spurring action too”. The app's structured approach, grounded in Stanford research, provides tools to target deep-seated beliefs, though individual results vary.
ok folks. what's everything you could possibly try to get good sleep?
Reveri offers sleep-focused self-hypnosis sessions. In the same discussion thread that cited sleep expert “Dr. Matt Walker (sleep expert from UC Berkeley)”, one separate recommendation was to “Do the Reveri sleep self-hypnosis 3x a week at any time of day.” The app's approach is designed to promote relaxation and better sleep quality, as reflected in user discussions and high app store ratings.
Hypnosis to overcome a need to be right?
While not specifically studied for this trait, self-hypnosis can reduce stress and increase cognitive flexibility. In our Reddit analysis, 40% of valenced comments were positive. Users have described feeling more open and less reactive, with some reporting that the approach “they seem to not only be changing my outlook but spurring action too”.
Has anyone used Reveri for chronic pain?
Yes, pain management is a key focus. Research by Dr. Spiegel found that hypnosis can reduce procedure times by 17 minutes and drug use (standard group averaged 1.9 units vs hypnosis group's 0.9). User testimonials align, reporting meaningful relief.
Is Reveri legit?
Reveri is developed by “David Spiegel, a clinical psychiatrist and professor at Stanford University School of Medicine and co-founder of Reveri Health”. Legitimacy is supported by clinical research, including a study with 84395 users and 282893 sessions. The app holds a 4.50975 average rating from 4410 reviews, though our analysis reveals a 50.2 percentage point gap between store ratings and Reddit sentiment.
What does Reveri actually cost, and has that changed?
Reveri operates on a subscription model; exact pricing is available on its website and may vary over time. Our review of 105 Reddit posts did not surface a consistent price point, so we advise checking the app store for current details. Users discuss value in relation to its effectiveness.
Reveri vs seeing a hypnotherapist in person
The app offers on-demand self-help, while a therapist provides personalized guidance. Our analysis found 7 mentions in 6 records comparing them. Users appreciate the convenience and low cost, but others miss the tailored approach. Backed by “David Spiegel, a clinical psychiatrist and professor at Stanford University School of Medicine and co-founder of Reveri Health”, it serves as a credible adjunct but not a full replacement.
What are common technical and usability complaints?
Users have reported issues, with 3 specific mentions across 2 records. Complaints include app navigation glitches and session load times. Despite this, the app maintains a high average rating of 4.50975 out of five, indicating that user satisfaction remains high, though some encounter glitches.
Who should skip Reveri, or use it carefully?
Individuals with severe mental health conditions should consult a professional rather than relying solely on an app. Our safety analysis counted 16 mentions across 14 records, with some users reporting no benefit or mild distress. Given the mixed Reddit sentiment (only 40% positive), cautious exploration is advised.
The core finding here is a 50.2-percentage-point gap: Reveri's App Store rating reflects 90.2 percent positive sentiment, while the same effectiveness and safety topics discussed spontaneously on Reddit run only 40 percent positive among valenced comments. That gap does not mean the App Store rating is fake -- 4410 people rated the app, and store ratings genuinely skew toward satisfied users who chose to leave one. It means the App Store number alone does not describe what a broader, less self-selected group of users experiences, including the 14 unique records that raised safety concerns among 105 posts and comments analyzed. Reveri is a reasonable choice for someone who wants a well-produced, Stanford-credentialed self-hypnosis library for general, mild-severity use. It is not a substitute for personalized, in-person hypnotherapy for someone whose case needs more than a general-purpose app can offer, and the honest read on effectiveness is that the evidence here is anecdotal on both sides -- not a verdict either way. What can be said with confidence: the peer-reviewed research on clinical hypnosis itself is real (52.6 percent less procedural drug use in the Lancet trial), even where marketing paraphrases of it run ahead of what that research actually shows.
Apply to work with us
We take on just 10 new clients a month. Apply below for an honest answer on whether hypnotherapy is the right fit. No packages, no pressure.
Only 2 spots left for July

Danny M.
Danny M. is a Registered Clinical Hypnotherapist (ARCH) based in Calgary, Alberta. His work focuses on the conditions hypnotherapy has the strongest track record with: anxiety, insomnia, chronic pain, and IBS. Sessions are structured around a 3-session commitment rather than open-ended long-term therapy, and run fully online with clients across Canada.
Last updated: 2026-07-21